
One of the primary reasons parents state for choosing to do extinction sleep training is to “help” their baby sleep better. In our society parents are bombarded with messages about the utmost importance of sleep to their baby’s development and well-being. This leads to panic and stress when babies don’t follow what our culture has decided they should do (yes, it’s culture, not biology we’re listening to here). So parents – tired and filled with anxiety – turn to extinction methods hoping to improve their baby’s sleep. Perhaps not too surprisingly, many parents report that it works. Their babies are sleeping better, happier, and then they turn around and tell the next sleep-deprived, stressed-out parent that they need to do the same thing to reap the rewards.
The question we have to ask ourselves is this: Is it working?
We have tons of parents reporting how much better their baby’s sleep is, they couldn’t possibly all be wrong could they? Babies must be sleeping better, right?
Well, it turns out the answer may actually be: No.
I can imagine the uproar of people telling their computer screens that they know tons of studies that support extinction sleep methods as being effective. They have read them, heard about them, and can quote them. I too have read them all (for a review of these studies, see
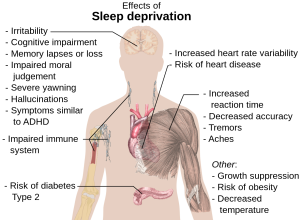
The objective measurement of sleep

Source: North Country Neurology
Yes, for years the only way we could measure sleep is to trust what parents reported. The problem with this is that parents can be wrong. Infants can wake up and not call out to us, letting us believe that they are sleeping through when in fact they are not. Depending on your reasons for using extinction sleep training methods, this can have serious consequences for your rationale. Luckily for us, two studies have come out recently that included objective measures of infant sleep using actigraphy data[2][3]. Even more interestingly, both of these studies set out to prove that these extinction methods improved infant sleep.
I’ll start with the Gradisar and colleagues paper[3] because it was a smaller study with only 43 families taking part (fewer who provided all data) split over three groups. The authors of this study included parental diary reports of sleep as well as actigraphy data to compare the two means of data collection on infant sleep habits. The authors spent a good deal of their paper discussing the benefits of extinction sleep training based on the parental reports; however, they had to add this in at the end: “No significant sleep changes were found by using objective actigraphy, suggesting sleep diaries and actigraphy measure different phenomena… further suggesting infants may still experience wakefulness but do not signal to parents.” (p. 6)
This is important because what the authors are saying is that there was no objective measure that infant sleep improved at all from the use of extinction sleep methods. These authors claim they believe it represents “self-soothing”, a claim that have rebutted with their own data in this summary here, but regardless, it makes it clear that their data does not support the notion of using extinction methods to improve our infants’ sleep.
The second study, from Wendy Hall and colleagues[2] is colloquially known as the “Rocky Mountain Sleep Study” and Dr. Hall is a very large proponent of pushing controlled crying on families starting at 6 months of age. Her goal is to help infant sleep and she believes these methods do just that. As acknowledged in the opening to this paper, it was reviewers of previous studies who requested objective measures of data be included to make comparisons. The current study looked at children aged 6-8 months and the families were randomly assigned to the different groups, ensuring a randomized controlled trial.
Now, it should be known that there are issues with this study more generally, such as the set up. In this study, the intervention group received both sleep information and the push to do controlled crying whereas the control group received information on infant safety, not the actual sleep information given to the intervention group. This means that the researchers would not be able to determine if any change was due to this additional information (and potential change in expectations) versus the actual extinction methods given to families. However, in terms of what we’re looking at – objective improvements in infant sleep – the data is there. With 117 infants in the intervention group and 118 in the control group, there was sufficient power to detect differences in sleep.
Again, like previous studies, the sleep diary information from parents supports the efficacy of the intervention, with parents reporting fewer night wakings and better sleep for their babies. Unfortunately for the hypothesis that extinction methods help infant sleep, the objective data does not support change. Actigraphy was used to assess number of night wakings (night wake episodes), long wake episodes, and longest sleep period both at intake and at the six-week follow-up. This is what was found:
- Night waking episodes. At baseline the intervention (controlled crying) group had an average of 8.2 night wakings while the control group had 8.8. At the six-week follow-up, the intervention group had an average of 7.9 night wakings and the control group had an average of 7.7. There was no statistical difference between the 7.9 and 7.7 and no analysis was conducted to see if the change was significant between the two groups (i.e., the intervention group change of 0.3 night wakings versus the control group change of 1.1 night waking episodes).
- Long wake episodes. Perhaps these are more important for parents because these are when we often get woken too. At baseline, the intervention group had an average of 4 long wake episodes compared to 4.2 for the control group. Both groups had an average of 3.2 long wake episodes at the six-week follow-up.
- Longest sleep duration. Here is where we get a near-significant difference that we’ll discuss. At baseline, the intervention group had an average longest stretch of 164 minutes which increased to 204.4 minutes at follow-up. The control group had an average longest stretch of 168 minutes at baseline which increased to 188.1 at follow-up. This difference had a p-value just at 0.05, which borders significance. So the controlled crying intervention may lead to a slight increase in the longest stretch. But how great is this difference? The practical difference here is 16.3 minutes which is doubtful to have any practical effects on infant sleep quality, though others may differ with my opinion on that.
Now, it is worth noting that the researchers stated they hypothesized change in infant sleep based on their intervention and focused their rationale for their intervention on the importance of adequate sleep for infants’ cognitive development. In the discussion, after concluding that there were no objective differences in sleep, the authors claim that “[b]ehavioral interventions are intended to assist infants to self-soothe back to sleep rather than to prevent night waking”. If you believe that children are actually learning “self-soothing” then I recommend you read this and this to help better understand the process of self-soothing and how it develops, but it was interesting to read the change in tune from what they expected to having to justify that they are not actually assisting infant sleep at all.
“But I swear my baby is happier now that he sleeps more!”
You will not be hard-pressed to find many families declaring that they see their child as happier and more engaged after using extinction sleep methods. These parents are certain their child is sleeping better and is therefore feeling better. What can we make of this? If we accept the objective data in front of us, in most cases (remember data doesn’t determine the outcome for everyone, but gives us generalities) there is no change in their infant’s sleep at all so what is going on?
Source: Wikipedia
Personally I think it’s as simple as understanding the parental mindset. We have to look to research on the factors that influence how we see the world to better understand how parents can see a change that might not have actually taken place. The first thing to consider here is that if parents are waking less because their children aren’t signalling to them, they may be better rested and therefore see the world through more rose-coloured lenses. There is ample evidence of the effects of sleep deprivation on cognition, but less discussed is the evidence that it negatively affects socio-emotional skills such as empathy and emotional intelligence[4], is associated with bias towards negative events[5], increases mood disturbances and emotional difficulties[6], and impairs the accurate recognition of emotions in others[7]. If we think about these skills in a mother who is struggling with sleep because either she has unrealistic expectations for sleep, there is an underlying issue for sleep for her infant, or there is something about her own health or ability to sleep that impedes sleep beyond what is normal for new parents, the effects of this sleep deprivation would lead her to view her infant in a different manner. She may not be as empathic and therefore view her child as more of a threat, she may not even accurately recognize the emotions her infant is presenting, or she may just be more biased at looking at any negative in the day. These would disappear after better sleep for her without her infant having changed anything at all.
Where do we go from here?
It would be silly to dismiss these possible positive effects for parents that they seem to be reaping from sleep training. However, we must first make sure parents are aware that sleep training is for them, not their babies. When we are able to focus on this fact, I firmly believe it opens us up to finding solutions that work for families while respecting our infants and their psychological (and very normal biological) needs for proximity and responsiveness during the night. I have said it before and I will say it again: We need more support for families.
For those mothers who are in the thick of it all and who are exhausted, please realize that extinction methods are likely not going to help your infant at all. So ask yourself what your end goal is for your child and then consider alternative means of getting there. Does this mean more support for you? Changing your expectations? Looking at alternatives for sleep, like co-sleeping? Figuring out what you need and how you can get that while providing the type of responsive caregiving your child needs is essential.
For those of you who have friends or family in the thick of it, don’t suggest they leave their child to cry. Please don’t. Instead take a look at how you can better support the parents in your life. Are you able to serve as help for a night so a tired parent can get a rest? Can you offer up a gift of a night doula? Can you take care of household chores so there’s one less thing to worry about? Cook meals and deliver them when times are tough, not just during the newborn period? Think long and hard about what you can do that truly supports not only the parents, but their baby too, and then do what you can, no matter how small it may seem.
____________________________
[1] Mindell JA, Kuhn B, Lewin DS, Meltzer LJ, Sadeh A. Behavioral treatment of bedtime problems and night wakings in infants and young children. Sleep 2006; 29: 1263-1276. [2] Hall WA, Hutton E, Brant RF, Collet JP, Gregg K, et al. A randomized controlled trial of an intervention for infants’ behavioral sleep problems. BMC Pediatrics 2015; 15: 181. [3] Gradisar M, Jackson K, Spurrier NJ, Gibson J, Whitham J, et al. Behavioral interventions for infant sleep problems: a randomized controlled trial. Pediatrics 2016; 137: e20151486. [4] Killgore WDS, Kahn-Greene ET, Lipizzi EL, Newman RA, Kamimori GH, Balkin TJ. Sleep deprivation reduces perceived emotional intelligence and constructive thinking skills. Sleep Medicine 2008; 9: 517-26. [5] Yoo SS, Gujar N, Jolesz FA, Walker MP. The human emotional brain without sleep—a prefrontal amygdala disconnect. Curr Biol 2007; 17: R877-R878. [6] Dinges DF, Pack F, Williams K, Gillen KA, Powell JW, et al. Cumulative sleepiness, mood disturbance, and psychomotor vigilance performance decrements during a week of sleep restricted to 4-5 hours per night. Sleep 1997; 20: 267-77. [7] van der Helm E, Gujar N, Walker MP. Sleep deprivation impairs the accurate recognition of human emotions. Sleep 2010; 33: 335-42.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
[…] Babies do not need sleep training. They know how to sleep. Society just does not like how it looks. It’s not tidy, it’s not straightforward, it’s cyclical and at times elusive. It’s not predictable and it doesn’t always allow the freedom and ease society likes it to have to allow the parents to get on with ‘more important’ work that isn’t the time spent helping their baby get the sleep they need in a manner that is normal for that baby. […]
[…] In fact, there is plenty of evidence that sleep training doesn’t result in better sleep, and many that do sleep train, end up having to do it over and over again after ‘leaps’ or periods of intense development occur. Tracy Cassells talks about whether sleep training works in a lot of detail on her website. […]
[…] THIS. if you read any, read this: evolutionaryparenting.com/helping-baby-sleep/ […]
If you are going to look at pediatric sleep, I might suggest looking at Dr. Douglas Teti’s work. While we still have a long road ahead of us in pediatric sleep research, he is doing great work that you might find interesting!
[…] Back to bedsharing. You may be thinking: bedsharing simply won’t work for me- my baby is loud, restless, and would constantly want to nurse. And to that I say, Congratulations! You have a normal, healthy baby! Not only is night waking normal and adaptive for our species, it reduces your child’s risk of SIDS and also means your chances of successful extended breastfeeding have greatly increased. Sleep researcher James McKenna notes, “From a biological perspective, it is appropriate for babies to awaken during the night during the first year of life. In fact, although infants can be conditioned to sleep long and hard alone, and hence, fulfill the cultural expectation that they should ‘sleep through the night’ the fact remains that they were not designed to do so, and it may not be either in their best biological or psychological best interest. ” In fact, research shows that just because your baby isn’t waking you up at night, doesn’t mean they’re still wa…. […]
[…] • https://gku.flm.mybluehost.me/evolutionaryparenting.com/helping-baby-sleep/ […]